
Key takeaways:
~ Up to 80% of women will experience hot flashes, or vasomotor symptoms (VMS), during menopause.
~ Research shows that changes in estrogen levels and activation of neurokinin 3 receptors in the hypothalamus are involved in triggering hot flashes.
~ Natural supplements and key lifestyle changes may help to reduce the intensity and duration of hot flashes.
Members will see their genotype report below, plus additional solutions in the Lifehacks section. Consider joining today.
What causes hot flashes?
Have you ever experienced a sudden wave of heat during menopause? You’re not alone. About 53-80% of women experience hot flashes around the time of menopause.[ref]
Hot flashes, or vasomotor symptoms, are a hallmark of the menopausal journey for many women. Hot flashes cause a sudden feeling of warmth, often accompanied by sweating and a flushed face. Some people also feel irritable and anxious during a hot flash. At night, hot flashes can cause night sweats and disrupt sleep.[ref]
What causes hot flashes? Why does the body’s temperature system seem to suddenly go haywire? Let’s dive into the science:
Biological causes of hot flashes:
While the exact cause of hot flashes is still not fully understood, several biological factors are thought to play a role.
Declining estrogen levels:
Women are born with a finite number of egg cells. As the number of eggs or follicles in the ovaries dwindles, estrogen levels will decline and the cyclical rise and fall of FSH (follicle-stimulating hormone) changes. This is called the menopausal transition or perimenopause.[ref]
The brain’s temperature control is sensitive:
The hypothalamus, a part of the brain, acts as the body’s thermostat. When estrogen levels drop, it can cause the body’s thermostat (the hypothalamus) to become more sensitive to slight changes in body temperature.
As estrogen levels decline during menopause, the hypothalamus may mistakenly sense that the body is overheating. In response, it triggers a series of events to cool the body down, resulting in the symptoms of a hot flash.
Cooling off by flushing:
To dissipate the perceived heat, blood vessels near the skin’s surface dilate. This causes flushing and sweating as the body tries to cool down.
Physiologically, what triggers the perceived temperature changes?
For years, doctors and researchers have known that the drop in estrogen is linked to hot flashes, but they didn’t know the exact mechanism. One known link was that hot flashes could be stopped by increasing estradiol, a form of estrogen. Therefore, it was thought that a lack of estrogen caused hot flashes.
New research in the last decade helps explain why changes in estrogen levels cause the brain to think the body is too hot, and what other neuropeptides are involved in triggering hot flashes.
Estrogen in the brain is part of the picture:
The hypothalamus is the region of the brain responsible for maintaining a stable body temperature through a series of feedback systems. This region receives sensory information from the periphery (the arms, legs, etc.) and also regulates the temperature of the brain. The hypothalamus also controls the circadian changes in body temperature throughout the day and night.[ref]
Estrogens are steroid hormones that act on receptors in the nucleus of cells to cause the transcription of a number of different genes. Estradiol (E2) is the major circulating estrogen in women prior to menopause, and it is synthesized primarily in the ovaries.[ref] Thermosensitive neurons have estradiol receptors and can suppress heat production and increase heat loss. But it’s not as simple as estrogen=heat. Instead, there are both inhibitory and excitatory effects of estrogen in the hypothalamus.[ref]
For example, higher estrogen levels in women are associated with sweating more easily when exercising. Core body temperature also fluctuates in response to changing estrogen levels during the menstrual cycle (e.g. warmer during ovulation).[ref]
In menopause, the overall decrease in estrogen is associated with hot flashes. Estrogen-sensitive neurons are involved, but estrogen isn’t the only cause of hot flashes.[ref]
Neurokinin B plays an important role:
In the hypothalamus, neurokinin B (NKB) signals to its receptor during hot flashes. This is an adaptation in response to sex steroid deficiency (decreased estrogen).
Neurokinin B is a neuropeptide involved in the release of gonadotropin-releasing hormone (GnRH) in the hypothalamus. It is important during pregnancy and puberty.
GnRH secretion is what drives the release of follicle-stimulating hormone (FSH) and luteinizing hormone (LH) in the menstrual cycle.[ref] In addition to estrogen declining, FSH and LH levels are also altered during menopause.
Here’s what researchers have learned recently about neurokinin B and hot flashes:
- Neurokinin B was identified in a genome-wide association study as the only gene that plays a significant role in hot flashes (vasomotor symptoms).[ref]
- Another strong indication that neurokinin B is integral to hot flashes is that when neurokinin B is given to young women by IV, it triggers hot flashes in 80% of the women.[ref]
- A placebo-controlled clinical trial of an NK3R (neurokinin B receptor) antagonist drug, which blocks the neurokinin B receptor, showed that it quickly reduced hot flash frequency by more than half compared to a placebo.[ref][ref]
The emerging picture is that hot flashes involve body temperature mechanisms in the hypothalamus that are affected by estrogen and neurokinin B, which in turn affect FSH and LH levels.
Acetylcholine and vasodilation:
In addition to what is going on in the brain with temperature control, women with hot flashes are likely to have an enhanced response to acetylcholine in small blood vessels. This means that the blood vessels are more likely to dilate rapidly due to the release of acetylcholine, causing the sweating and flushing associated with hot flashes.[ref]
A clinical trial of an anticholinergic drug found that it was superior to placebo in reducing hot flashes. Anticholinergic drugs block acetylcholine.[ref]
Environmental factors that increase hot flashes:
Phthalates: endocrine disruptors and increased hot flashes
Phthalates are a class of chemicals used in cosmetics, shampoos, vinyl products, artificial fragrances, nail polish, deodorants, and lotions. They are ubiquitous, meaning that pretty much everyone is exposed to them these days. Phstalates can act as endocrine disruptors or estrogen mimics. A recent study showed that women who had higher phthalate levels in their system were about 45% more likely to have hot flashes. [ref] Multiple studies replicate this association of phthalates with hot flashes.[ref][ref]
High CO2 levels:
When you hold your breath, CO2 levels rise, and an increase in CO2 levels can trigger hot flashes in menopausal women.
A study in healthy menopausal women used a brief CO2 exposure of a single inhalation of 20% or 35% CO2. This mimics the increase in CO2 seen during panic attacks, anxiety, or breath-holding. The majority of the menopausal women experienced a hot flash within minutes of inhaling 20% CO2.[ref]
Chronic inflammation and more intense hot flashes:
Researchers have found that the intensity of hot flashes is associated with higher levels of inflammatory cytokines (IL-8 and TNF-alpha). According to the authors: “These results suggest that hot flashes are linked to low-grade systemic inflammation in postmenopausal women.”[ref]
Leaky gut and hot flashes:
Another study found that hot flush intensity may be related to increased intestinal barrier permeability (also known as leaky gut). Estrogen levels affect the gut microbiome and may cause higher levels of gut permeability. This, in turn, causes low-grade systemic inflammation.[ref]
Spicy foods, hot rooms:
While not a direct biological cause, certain external factors can trigger or worsen hot flashes. These include alcohol, caffeine, spicy foods, tight clothing, heat, and stress.
Smoking:
Cigarette smoking increases the odds of hot flashes by 6-fold.[ref] This may be through the interaction with the aryl hydrocarbon receptor and estrogen metabolism as well as increased inflammatory cytokines.
What isn’t linked to hot flashes?
- Research shows that a higher BMI is not associated with an increased risk of hot flashes.[ref]
- Cortisol and the cortisol awakening response are likely not involved in hot flashes, according to researchers.[ref]
What about men? Can they get hot flashes?
While hot flashes are commonly associated with menopause in women, men can also experience them, especially those undergoing certain medical treatments, such as hormone therapy for prostate cancer. The biological mechanisms in men may be similar, involving changes in hormone levels and the body’s temperature regulation system.
Genotype Report
TACR3 gene:
Encodes the neurokinin B receptor, which was identified in multiple genome-wide studies as the most significant gene affecting hot flashes. Note that other variants in TACR3, which are not included in 23andMe or AncestryDNA data, can also increase or decrease the risk of hot flashes.
- C/C: most common genotype, higher risk of hot flashes
- C/T: decreased risk of hot flashes
- T/T: significantly decreased risk of hot flashes[ref][ref]
Members: Your genotype for rs77322567 is —.
CYP1B1 gene:
Encodes a phase I detoxification enzyme involved in estrogen metabolism. The CYP1B1 enzyme is responsible for one of the ways that estrogen can be broken down and eliminated.
Check your genetic data for rs1800440 (23andMe v4; AncestryDNA):
- C/C: 3-fold greater odds of experiencing hot flashes for more than a year[ref]
- C/T: typical risk
- T/T: typical (most common genotype)
Members: Your genotype for rs1800440 is —.
AHR gene:
Encodes the aryl hydrocarbon receptor, which in turn affects CYP1B1 and estrogen metabolism. The aryl hydrocarbon receptor is also activated by cigarette smoke and air pollution, possibly connecting both of those to hot flash frequency and intensity.
Check your genetic data for rs2066853 (23andMe v4; AncestryDNA):
- G/G: typical
- A/G: typical risk
- A/A: increased risk of hot flashes[ref]
Members: Your genotype for rs2066853 is —.
COMT gene:
Encodes the catechol O-methyltransferase enzyme which is involved in the phase II metabolism of certain estrogen metabolites.
Check your genetic data for rs4680 Val158Met (23andMe v4, v5; AncestryDNA):
- G/G: Val/Val – fast (higher) COMT activity[ref]
- A/G: Val/Met – intermediate COMT activity (most common genotype in Caucasians); typical risk
- A/A: Met/Met – slow (40% lower COMT activity)[ref] in current smokers, a 13-fold increased risk of hot flashes[ref]
Members: Your genotype for rs4680 is —.
SULT1A1 gene:
Encode sulfotransferase 1A1, an enzyme involved in the conversion of an estradiol metabolite.
- T/T: typical
- C/T: one SULT1A1*3 allele, decreased risk of hot flashes
- C/C: SULT1A1*3 , decreased risk of hot flashes[ref]
Members: Your genotype for rs1801030 is —.
Lifehacks: Natural hot flash relief
Natural lifestyle, diet, and herbal supplement options can help reduce hot flashes, and here are some of the research-backed solutions. While research studies don’t cover every natural treatment, they give us a good starting point for knowing what’s more likely to work.
Talk with your doctor about prescription medications and hormone replacement therapy (HRT) options for hot flashes. There are several options, but medications come with some risks and aren’t right for everyone.
Lifestyle changes to reduce hot flashes
Avoid phthalates as much as possible:
A number of studies show a strong link between higher levels of phthalates in the body and increased numbers of hot flashes.
Phthalates are found in many products, but a big source for women is personal care products. Look for lotions, shampoos, conditioners, and cosmetics that are phthalate-free. Another big source is artificial fragrances, such as those found in laundry products or air fresheners. Look for fragrance-free options.
Women who have lower levels of phthalates in their urine have fewer hot flashes on average.[ref] Read more about phthalates, genetics, and how they are metabolized.
Breathe:
The study on CO2 triggering hot flashes provides insight into how stressful situations can cause a hot flash, as many people naturally hold their breath when stressed. Breathing exercises can help you avoid instinctively holding your breath in a stressful situation. Look into box breathing, physiological sighing, or yoga breathing to help control your breathing.
Some research suggests that wearing a mask increases hot flashes. Wearing an N95 mask also increases CO2, but not as much as holding your breath. It may be that masking increases hot flashes due to the increase in heat on the face from the mask or due to increased CO2 levels.[ref]
Related article: Anxiety and Genetics (read the part about the CO2 sensing gene)
Dietary interventions:
A recent study found that a low-fat, plant-based diet with minimal oils helped reduce moderate to severe hot flashes. The intervention also included the daily consumption of cooked, non-GMO soybeans. Looking at the details of the dietary changes, fat intake decreased by about 50% and fiber intake increased by 12g/day.[ref] There were several changes taking place in the study (eating soy, increasing fiber, and decreasing fat), which makes it difficult to know which component was effective(e.g. avoiding nuts, eating soy, or avoiding animal-derived foods).[ref]
Gut healthy diet:
The link between changing estrogen levels and the gut microbiome makes gut health a priority. What does a gut health diet look like? There are dozens of different types of diets that are promoted as healthy – from Mediterranean to DASH to Paleo. One thing they all have in common is that they cut out processed, packaged foods and focus on eating whole foods. Microbiome studies show that cutting out processed foods can help with gut health.[ref]
Related article: Emulsifiers, IL-10, and Leaky Gut
Research on natural supplements and drugs for hot flashes:
Below are some of the research studies on solutions for reducing hot flashes. Key here is that there are multiple options for reducing hot flashes, both natural supplements and prescription medications. Talk with your doctor for medical advice about what may work best for you, and if you’re taking supplements, be sure to ask about any drug interactions with what you’re taking.
Prescription medications used for hot flashes:
Hormone therapy:
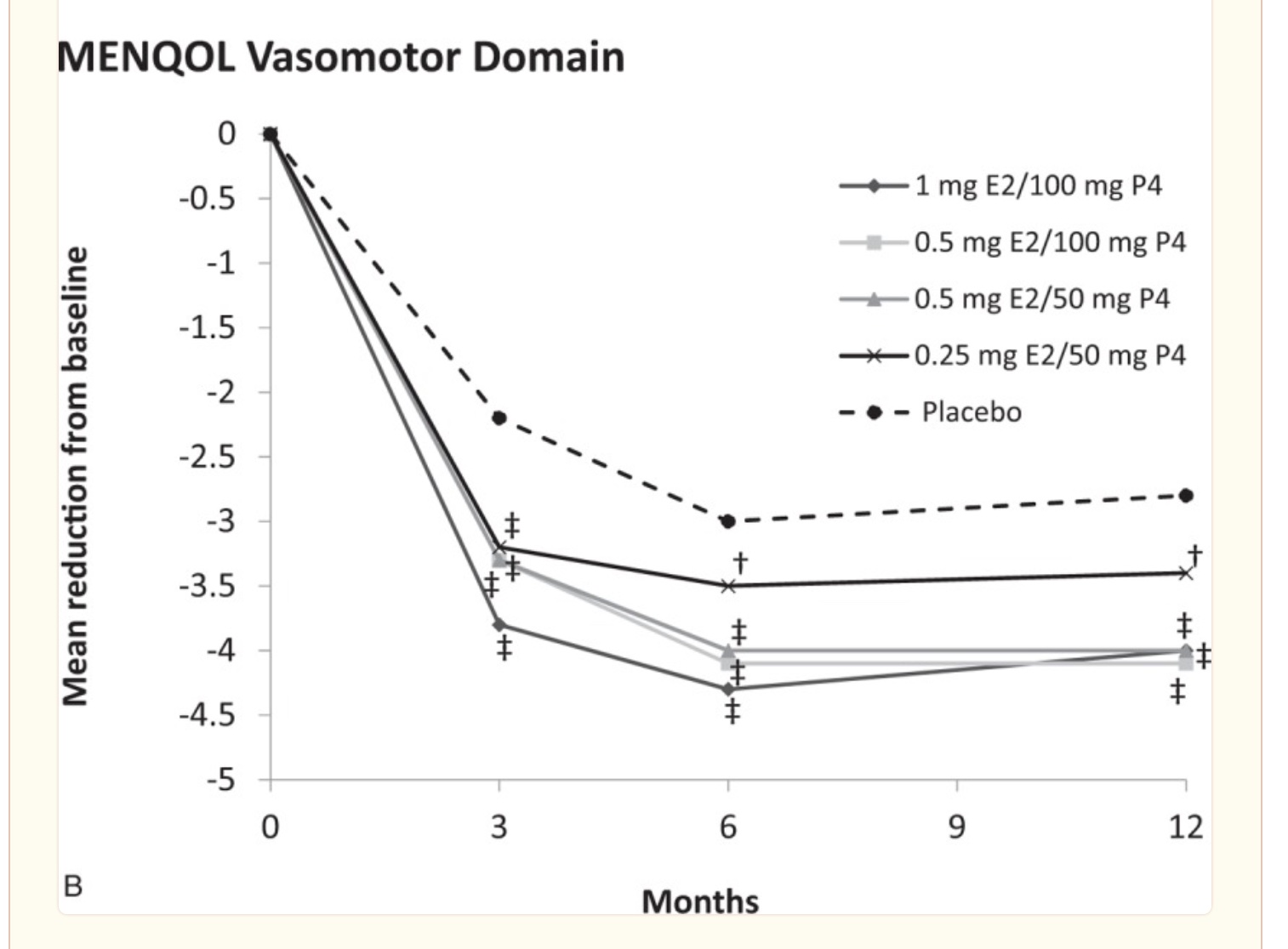
Hormone replacement therapy (HRT) is often considered the gold standard for treating hot flashes. In clinical trials, estrogen or estrogen plus progesterone works to reduce hot flashes more than a placebo.[ref]
Who is more likely to benefit from HRT?
A study of 150 menopausal women found that hormone therapy (estrogen or estrogen plus progesterone) helped with menopausal symptoms, including hot flashes. However, the positive benefits were only seen in women who had hot flashes at the start of the study. In the group of women who didn’t have hot flashes, there was no benefit from hormone therapy for menopausal symptoms.[ref]
Talk with your doctor to get a full picture of the pros and cons of hormone therapy, taking into account your medical and family history of heart disease or estrogen-related cancers.
A 2019 meta-analysis found that HRT increased the relative risk of estrogen-receptor-positive breast cancer. The increase in risk depended on the timing, weight of the women, and type of hormone used. For example, normal-weight women were at an increased risk of breast cancer, but overweight women had little excess risk.[ref] Weigh that risk against possible benefits for cardiovascular health[ref] and possible risks of blood clots or stroke.[ref]
SSRIs and SNRIs:
Other options that doctors may prescribe for hot flashes are SNRIs and SSRIs, such as venlafaxine and escitalopram.[ref] Studies do show that they are statistically more effective than placebo.[ref]
Neurokinin 3 receptor antagonist, fezolinetant:
A clinical trial on neurokinin 3 receptor antagonists shows that they are statistically likely more effective than SNRIs.[ref] This type of drug was approved by the FDA in May 2023 for hot flashes.[ref]
Natural supplements for reducing hot flashes:
Curcumin:
A placebo-controlled clinical trial of curcumin found that it reduced the frequency of hot flashes after four weeks.[ref] Curcumin helps to reduce chronic inflammation, so it may work best for someone with higher TNF-alpha or for someone with a chronic inflammatory disease.
Related article: TNF-alpha genetic variants.
Saffron:
A placebo-controlled trial of saffron extract (15mg/twice daily) found that it reduced hot flashes in menopausal women.[ref] Saffron has been traditionally used as a spice and natural medicine with records of its use dating back to the 12th century BC. In addition to antimicrobial activity, saffron also shows neuroprotective effects and may increase GABA, the inhibitory neurotransmitter.
Isoflavones (phytoestrogens):
An analysis of 17 clinical trials on isoflavones (e.g. soy, red clover) found that increased isoflavone intake was likely effective for hot flashes. However, amino acid supplements had no effect.[ref] Similar to hormone therapy, talk with your doctor about the pros and cons of phytoestrogens and any family history of estrogen-related cancers.
Valerian root:
A placebo-controlled study showed that valerian root reduced the frequency of hot flashes.[ref] Valerian root is known for reducing feelings of anxiety, so it may be more effective for women with hot flashes along with anxiety/irritability.
St. John’s wort:
A placebo-controlled trial of St. John’s wort for menopausal symptoms showed that it was statistically effective in reducing the intensity and frequency of hot flashes.[ref] However, another trial of St. John’s wort and Vitex agnus-castus found that they had no significant effect on hot flashes.[ref]
Trials with negative results:
The following studies found no significant benefit for the following interventions. Remember that what doesn’t work for a group of women may still work for an individual. However, knowing what is less likely to work can help you prioritize what to try first.
DHEA:
A meta-analysis of data from 16 clinical trials concluded that DHEA did not significantly affect hot flashes or menopausal symptoms (but it may increase androgenic side effects, such as acne).[ref]
Acupuncture:
A meta-analysis that included data from several studies found that acupuncture does not decrease the frequency or intensity of hot flashes. However, it was effective for other menopausal symptoms.[ref]
Aerobic exercise or yoga:
A study using sleep monitors found that neither aerobics nor yoga had a detectable effect on hot flashes or sleep in menopausal women.[ref]
Omega-3 fatty acids:
A clinical trial of 1.8 g of omega-3s daily for 12 weeks showed no effect on vasomotor symptoms or sleep quality.[ref]
Black cohosh:
Study results are mixed for the herbal supplement black cohosh for hot flashes. However, a meta-analysis that combined data from 16 studies found that black cohosh was unlikely to reduce hot flashes.[ref]
Recap of your genes:
| Gene | RS ID | Effect Allele | Your Genotype | Notes About Effect Allele |
|---|---|---|---|---|
| TACR3 | rs77322567 | T | — | decreased risk of hot flashes |
| CYP1B1 | rs1800440 | C | — | C/C: 3-fold greater odds of experiencing hot flashes for more than a year |
| AHR | rs2066853 | A | — | A/A: increased risk of hot flashes |
| COMT | rs4680 | A | — | A/A: in current smokers, a 13-fold increased risk of hot flashes |
| SULT1A1 | rs1801030 | C | — | SULT1A1*3 , decreased risk of hot flashes |
[/mepr-show]
Related Articles:
About the Author:
Debbie Moon is the founder of Genetic Lifehacks. Fascinated by the connections between genes, diet, and health, her goal is to help you understand how to apply genetics to your diet and lifestyle decisions. Debbie has a BS in engineering and also an MSc in biological sciences from Clemson University. Debbie combines an engineering mindset with a biological systems approach to help you understand how genetic differences impact your optimal health.