
The MTHFD1 gene encodes the methylenetetrahydrofolate dehydrogenase enzyme, which is an essential part of the folate cycle. It’s a trifunctional enzyme that catalyzes three sequential reactions in the folate cycle, which is essential for DNA synthesis, DNA repair, and DNA methylation.
Function of MTHFD1:
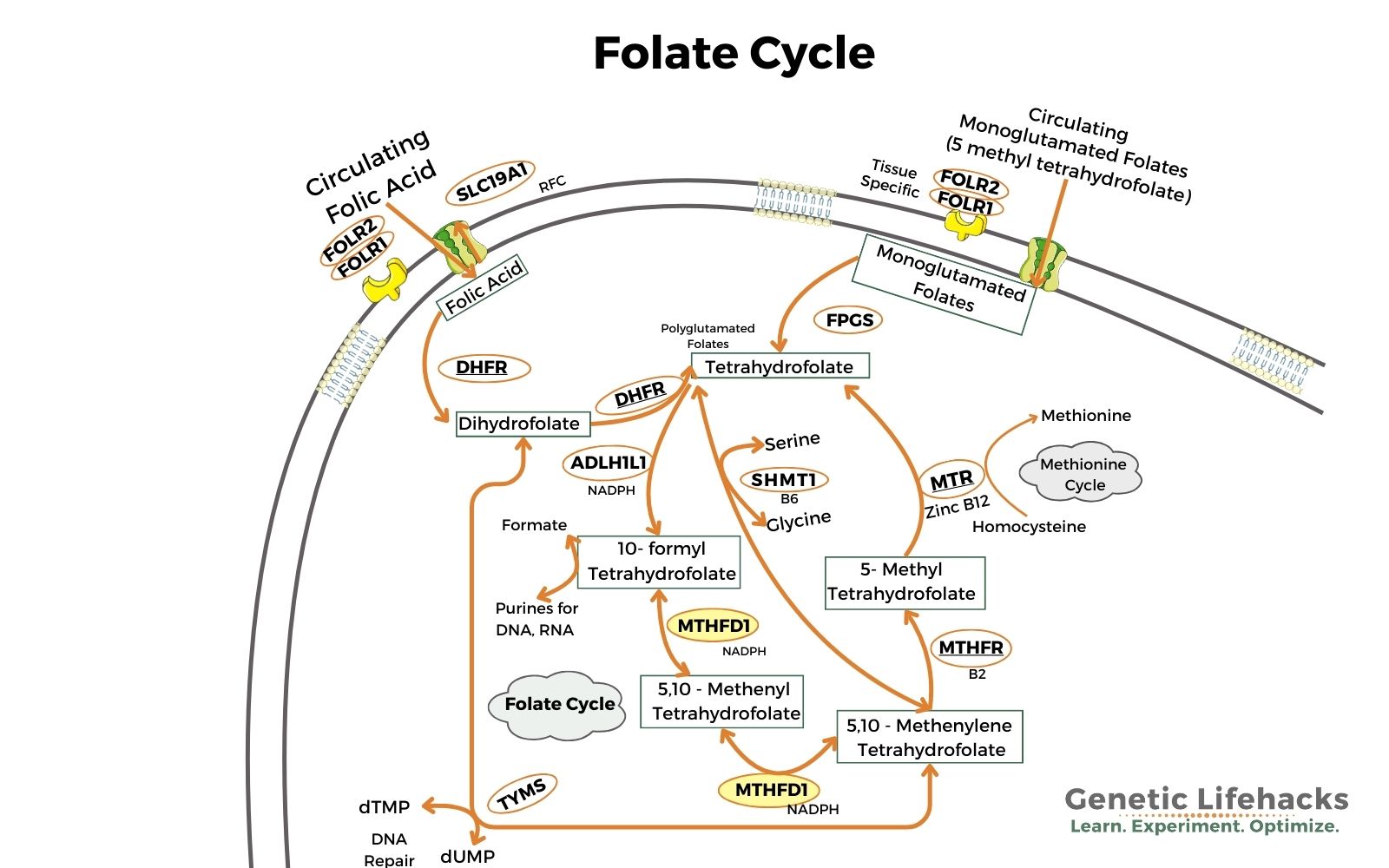
The MTHFD1 enzyme acts within the folate cycle to convert 5,10-methylenetetrahydrofolate to 5,10-methenyltetrahydrofolate and converts 5,10-methenyltetrahydrofolate to 10-formyltetrahydrofolate.
This needs a diagram:
How does the body use folate?
Folate is used in multiple pathways in the body:
- It is used in creating the purine nucleotides needed for DNA and RNA
- Serine and glycine need folate for the interconversion
- Folate is important in the methylation cycle, creating methyl groups,
- Methyl groups are important in the detoxification of arsenic, the creation of melatonin from serotonin, and the metabolism of histamine (plus many other reactions!).
Severe deficiency:
MTHFD1 is an essential part of the cellular process for making some of the nucleotides needed for DNA and RNA. There are only a handful of known case studies on more severe MTHFD1 deficiency, and from these studies, we can get an idea of how important MTHFD1 is (and why complete deficiency isn’t compatible with life).
The studies show that a more severe deficiency can lead to hyperhomocysteine, megaloblastic anemia, hemolytic uremic syndrome (HUS), severe combined immunodeficiency, and retinopathy. According to the case studies “all except the retinopathy resolved after treatment with hydroxocobalamin, betaine and folinic acid.”[ref]
MTHFD1 in pregnancy:
Genetic variants in MTHFD1 affect the relative risk of neural tube defects and other birth defects. Keep in mind that the increase in risk here is an increase in relative risk. This means that if the odds of neural tube defects are 1 in 10,000, then a variant that doubles the risk would make the odds 2 in 10,000. Still rare, but the research here points to the important role of folate in pregnancy.
Genetic variants in MTHFD1 in the mother are linked to increased relative risk of birth defects, congenital heart defects, and preterm birth.[ref][ref][ref] Folic acid has been recommended for decades for pregnancy because folate is essential for the proper development of the fetus. More recently, people with MTHFR and DHFR variants may opt for methylfolate, which is the more active form used by cells.
While more folate is needed during pregnancy, very high doses may backfire for people with MTHFD1 variants. A mouse model of MTHFD1 polymorphism was used in a study using high doses of folic acid (5X normal dose) during pregnancy. The study found: “Moderately higher folate intake and MTHFD1-synthetase deficiency in pregnant mice result in a lower methylation potential in maternal liver and embryos and a greater incidence of defects in embryos… These findings have implications for women with high folate intakes, particularly if they are polymorphic for MTHFD1 R653Q.”[ref]
MTHFD1 R653Q is rs2236225 (see genotype report below)
Choline takes up the slack:
In the methylation cycle, either choline or folate can be used as a source of methyl groups, and supplying choline from the diet takes the strain off the methylation cycle. For people with MTHFD1 variants, several studies show that getting more choline can mitigate the negative effects of the SNP.
For example, a study showed that people with the G1958A variant were 7-fold more likely to develop choline deficiency after a month on a diet low in choline. Essentially, carrying the variant means that someone needs about 8g of choline a day compared to 4g without the polymorphism. [ref]
Genotype report: MTHFD1
Member Content:
Why join Genetic Lifehacks?
~ Membership supports Genetic Lifehack’s goal of explaining the latest health and genetics research.
~ It gives you access to the full article, including the Genotype and Lifehacks sections.
~ You’ll see your genetic data in the articles and reports.
Join Here
Lifehacks:
If you carry the MTHFD1 variant, track your diet for a week or so to see how much choline and folate you eat. Be realistic – and if you aren’t exceeding the minimal choline and folate recommendations, consider supplementing or increasing choline and folate in your diet.
Increasing folate:
The US RDA for folate is 400 mcg of dietary folate equivalents, and the recommended upper limit is set at 1,000 mcg/day.
Methylfolate is the active form of folate that is available over the counter as a supplement. It has several advantages over folic acid, especially for people with MTHFR or DHFR variants. Folinic acid is another supplemental form of folate that may be beneficial for people with MTHFD1 variants. Both methylfolate and folinic acid are more readily useable in cells than dietary folate, which must be converted in the intestines. Keep this in mind when looking at supplements – you may not need as much methylfolate or folinic acid to reach your daily goal.
Focusing on increasing folate-rich foods is another way to mitigate the effects of MTHFD1.
| Food | Serving size | Folate (mcg) |
| Edamame | 1/2 cup | 241 mcg |
| Beef liver | 1 slice (81g) | 211 mcg |
| Lentils | 1/2 cup | 178 mcg |
| Chicken liver pate’ | 1/4 cup | 166 mcg |
| Chicken liver, pan-fried | 1 oz | 157 mcg |
| Black beans, cooked | 1/2 cup | 127 mcg |
| Broccoli, cooked | 1/2 cup | 84 mcg |
| Hummus | 1/2 cup | 73 mcg |
| Pinto beans, canned | 1/2 cup | 72 mcg |
| Black-eyed peas, canned | 1/2 cup | 61 mcg |
| Spinach, raw | 1 cup | 58 mcg |
| Brussels sprouts, cooked | 1/2 cup | 47 mcg |
| Green peas, canned | 1/2 cup | 37 mcg |
| Kidney beans, canned | 1/2 cup | 26 mcg |
| Green beans, canned | 1/2 cup | 21 mcg |
| Ribeye steak | 300 g | 19 mcg |
| Kale, raw | 1 cup | 19 mcg |
Choline:
Research shows that getting plenty of choline is important for people with the MTHFD1 G1958A variant. Carriers of the A allele are more likely to have choline deficiency on a low choline diet (modified by folate intake).[ref][ref] In one study with premenopausal women, those with an A-allele were 15 times more likely to show choline deficiency symptoms on a diet low in choline.
Choline intake is even more important for pregnant or breastfeeding women with MTHFD1 variants. One study found that women with either PEMT variants or MTHFD1 variants would benefit from higher choline intakes.[ref]
| Food | Mg per serving |
Percent DV |
|---|---|---|
| Beef liver, pan-fried, 3 ounces | 356 | 65 |
| Egg, hard-boiled, 1 large egg | 147 | 27 |
| Beef top round, separable lean only, braised, 3 ounces | 117 | 21 |
| Soybeans, roasted, ½ cup | 107 | 19 |
| Chicken breast, roasted, 3 ounces | 72 | 13 |
| Beef, ground, 93% lean meat, broiled, 3 ounces | 72 | 13 |
| Fish, cod, Atlantic, cooked, dry heat, 3 ounces | 71 | 13 |
| Mushrooms, shiitake, cooked, ½ cup pieces | 58 | 11 |
| Potatoes, red, baked, flesh and skin, 1 large potato | 57 | 10 |
| Wheat germ, toasted, 1 ounce | 51 | 9 |
| Beans, kidney, canned, ½ cup | 45 | 8 |
| Quinoa, cooked, 1 cup | 43 | 8 |
| Milk, 1% fat, 1 cup | 43 | 8 |
| Yogurt, vanilla, nonfat, 1 cup | 38 | 7 |
Meat and eggs are the most abundant sources of choline — but even so, a serving of chicken breast gives you 13% of the recommended daily value.
In short, if you want to know how much choline you normally get in your diet, you should track what you eat for a week or so. The free online app, cronometer.com, includes the choline content of foods. Choline content isn’t enabled by default, so you will need to go into the settings and turn on ‘choline’.
Recap of your genes:
| Gene | RS ID | Effect Allele | Your Genotype | Notes About Effect Allele |
|---|---|---|---|---|
| MTHFD1 | rs2236225 | A | — | decreased MTHFD1 enzyme stability, more of a reliance on choline as a methyl donor, increased relative risk of neural tube defects, slightly decreased risk of leukemia and cancers; increased relative risk of acute myocardial events |
| MTHFD1 | rs1076991 | T | — | minor decrease in enzyme activity, adds to decreases caused by other variants, increased relative risk of acute myocardial events |
| MTHFD1 | rs1950902 | G | — | G/G: increased relative risk of congenital heart defects in offspring |
Related articles and topics:
About the Author:
Debbie Moon is the founder of Genetic Lifehacks. Fascinated by the connections between genes, diet, and health, her goal is to help you understand how to apply genetics to your diet and lifestyle decisions. Debbie has a BS in engineering from Colorado School of Mines and an MSc in biological sciences from Clemson University. Debbie combines an engineering mindset with a biological systems approach to help you understand how genetic differences impact your optimal health.
It’s my first time on your blog, and I have to admit that I’m amazed at how much research you did to produce such a fantastic post. A important portion was built with the help of someone.
My brother suggested I might like this website He was totally right This post actually made my day You cannt imagine just how much time I had spent for this information Thanks
Your blog is a constant source of inspiration for me. Your passion for your subject matter shines through in every post, and it’s clear that you genuinely care about making a positive impact on your readers.
This blog is also fantastic. It loads your webpage quite swiftly. Which web host do you employ? Could you please share your affiliate link with me? My page should load just as quickly as yours does.